Health plans today operate in one of the most data-rich environments in healthcare history. Longitudinal claims data, CAHPS survey responses, quality measure files, outreach histories, enrollment details, care management notes, risk scores, and predictive analytics, all flow in continuously. By any measure, the data foundation has never been stronger.
Yet care gap closure rates remain stubbornly flat for many organizations. Enrollment in care management programs often levels off at 15–25%. Unsuccessful contact rates hover between 50–70%. Care teams dedicate too much time to repeated outreach attempts rather than meaningful interventions. STARS improvements come in small increments, and justifying ROI grows harder each year.
This disconnect prompts an obvious question: With richer data than ever, why aren’t care gap performance and Stars results advancing at the same pace?
The short answer: The limitation isn’t a lack of data. It’s an activation gap; the difficulty turning those existing signals into prioritized, timely, engagement-focused actions.
The Illusion of the Missing Data Problem
When enrollment stalls or contact rates stay high, the instinctive response is to seek additional inputs: better SDoH coverage, richer enrichment layers, new data vendors, or deeper member context. SDoH factors certainly refine targeting, and many plans have made substantial investments there. But even those that integrate SDoH effectively still face persistent challenges, viz., flat conversion rates, high unsuccessful contacts, operational drag, limited ROI attribution, and exhausted care teams.
The core issue rarely lies in missing information. It lies in the inability to convert the signals already in hand into decisions that respect member behavior and likelihood to engage.
Defining the Activation Gap
Traditional care management programs excel at one question: Who qualifies? Eligibility logic based on claims data flags members with open care gaps or rising risk. That step is necessary, but insufficient for scale.
What matters operationally is a different set of questions:
- Who is most likely to engage right now?
- Which members warrant priority this week?
- Which channel will reach them fastest and most effectively?
- Which individuals are unlikely to respond no matter how many attempts?
- Where is outreach effort being wasted?
Most programs optimize for volume and not for yield. Large eligibility lists feed sequential outreach. Conversion gets measured after the fact. Feedback loops are slow. The outcome is predictable friction: wasted calls, burned-out teams, and incremental Stars gains.
The Signals Already Exist
The encouraging reality is that most health plans already possess the key data streams needed to bridge this gap. When thoughtfully combined, three primary sources deliver powerful decision intelligence:
- Claims Data — Beyond static risk scoring or retrospective reporting, longitudinal claims reveal dynamic patterns: rising risk trajectories, growing reliance on emergency rooms, signs of medication non-adherence, fragmented care, provider switching, and preventive service gaps. This shifts focus from “who is high-risk” to “who is rising-risk and time-sensitive,” where timing directly influences impact.
- CAHPS Feedback — Often treated primarily as a compliance tool for Stars performance, CAHPS holds rich behavioral signals: levels of trust in providers, effectiveness of communication, perceived access barriers, care coordination frustrations, and navigation difficulties. These serve as leading indicators of engagement potential or resistance, enabling smarter differentiation between clinically eligible members who are reachable versus those who may be fatigued or disengaged.
- Outreach Logs — Historical outreach records are frequently underutilized beyond basic reporting. Yet they contain gold: preferred contact channels, optimal times of day, signs of channel fatigue, patterns among repeat non-responders, and sequencing effectiveness. When properly modeled, this history predicts future responsiveness rather than merely documenting past attempts.
Taken individually, these sources support reporting. Integrated, fuel prioritization and optimization.
A Practical Example: Medication Adherence Outreach
Consider medication adherence programs for Medicare Advantage plans, targeting Part D Stars measures such as statins, renin-angiotensin system antagonists (RAS antagonists), and diabetes medications.
Most plans routinely identify members with Proportion of Days Covered (PDC) below thresholds and launch outreach campaigns. Eligibility comes straight from claims data—that part functions well.
In practice, however, challenges emerge:
- Many members remain unreachable despite multiple attempts.
- Some have already refilled before outreach lands.
- Others have intentionally discontinued due to side effects.
- A recurring group appears on outreach lists quarter after quarter.
- Care managers invest significant effort in low-probability contacts.
The problem isn’t spotting the adherence gap; it’s distinguishing responsiveness profiles:
- Members who forgot to refill and are highly reachable.
- Those frustrated by side effects and less responsive.
- Individuals who prefer pharmacy text reminders over phone calls.
- Cases driven by access barriers rather than lack of intent.
Claims identify the issue. But layering in CAHPS (e.g., poor provider communication scores) and outreach history (e.g., SMS responders vs. phone avoiders, timing patterns) enables prioritized, channel-optimized outreach.
High-probability, high-engagement members get contacted first via preferred methods. Resistant cases route to pharmacist-led interventions. Chronic non-responders shift to automated or lower-touch approaches.
The outcome? Fewer wasted efforts, higher refill rates, more efficient use of care manager and pharmacist time, and stronger Starsperformance—without expanding headcount. No new data vendors required, just smarter activation of what’s already available.
Signal Activation Maturity Model
Organizations typically evolve through four stages of activation maturity.
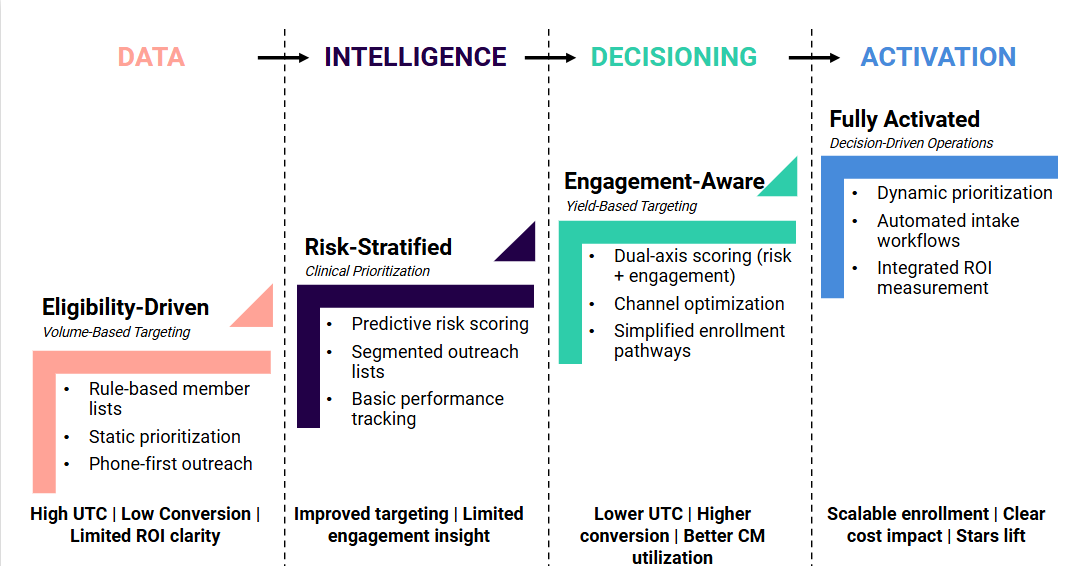
Most organizations operate between Levels 1 and 2. Competitive advantage lies in progressing toward Levels 3 and 4.
How MathCo Enables Signal Activation at Scale
Bridging the activation gap demands more than refreshed models—it requires an integrated approach spanning data, analytics, workflows, and outcomes tracking.
At MathCo, we partner with health plans to operationalize this through targeted capabilities:
- AI-Driven Risk & Engagement Stratification: We combine claims, CAHPS, and outreach history into dual-axis models that pinpoint high-impact, high-conversion opportunities.
- Intelligent Outreach & Channel Optimization: Predictive selection and sequencing to minimize unsuccessful contacts and maximize yield.
- Enrollment Acceleration & Workflow Automation: Digital pathways and automated validation to reduce friction and speed engagement.
- Integrated Measurement & ROI Visibility: Frameworks linking enrollment gains to utilization changes, cost reductions, and Stars improvements for credible ROI stories.
Our emphasis remains on activating embedded intelligence within existing systems, rather than chasing additional data layers.
The Strategic Imperative
The next generation of care management leaders will not differentiate based on who has the most comprehensive SDoH coverage. They will differentiate based on who can convert signals into faster, more precise operational decisions with clear, measurable results.
The future of care gap performance will not be defined by data accumulation. It will be defined by activation.
For health plans facing pressure to boost enrollment, streamline operations, strengthen medication adherence, improve CAHPS-driven experience metrics, and demonstrate sustainable ROI, the direction is straightforward:
You don’t need more data.
You need smarter activation!